Oxygen can be added by hooking the valve up to an
oxygen supply. Since the rescuer’s breath dilutes the
oxygen flow in artificial ventilation, adjust the flow
rate to increase oxygen concentration. At 5 liters per
m i n u t e , t h e o x y g e n c o n c e n t r a t i o n w i l l b e
approximately 50 percent. At 15 liters per minute, this
concentration will increase to 55 percent.
The mask has an elastic strap so it can be used on
conscious, self-ventilating patients to increase oxygen
concentration.
SUCTION DEVICES
The patient’s airway must be kept clear of foreign
materials, blood, vomitus, and other secretions.
Materials that remain in the airway may be forced into
the trachea and eventually into the lungs. This will
cause complications ranging from severe pneumonia
to a complete airway obstruction. Use suction to
remove such materials.
In the field, a Hospital Corpsman may have access
to a fixed (installed) suction unit or a portable suction
device. Both types of suction devices are equipped
with flexible tubing, suction tips and catheters, and a
non-breakable collection container.
Maintenance of suction devices consists of testing
the suction pressure regularly and cleaning the device
after each use.
Before using a suction device, always test the
apparatus. Once the suction pressure has been tested,
attach a suction catheter or tip. Position the patient on
his side, and open the patient’s mouth. This position
permits secretions to flow from the patient’s mouth
while suction is being delivered. Use caution in
patients with suspected neck or spinal injuries. If the
patient is fully and securely immobilized on a
backboard, the backboard may be tilted to place the
patient on his side. If you suspect such injuries but the
patient is not immobilized, suction as best you can
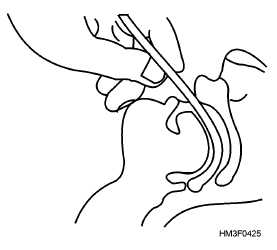
without turning the patient. Carefully insert the suction
tip or catheter at the top of the throat (fig. 4-25). DO
NOT push the tip down into the throat or into the
larynx. Apply suction, but for no more than a few
seconds, since supplemental oxygen or ventilations
cease while suctioning, keeping oxygen from the
patient. Suction may be repeated after a few breaths.
CRICOTHYROIDOTOMY
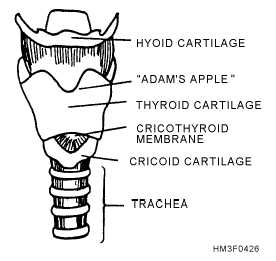
A cricothyroidotomy, often called an emergency
tracheotomy, consists of incising the cricothyroid
membrane, which lies just beneath the skin between
the thyroid cartilage and the cricoid cartilage. In most
cases, the cricothyroid membrane can be easily located
by hyperextending the neck so that the thyroid notch
(Adam’s apple) becomes prominent anteriorly.
Identify the position of the thyroid notch with the index
finger. This finger descends in the midline to the
prominence of the cricoid cartilage. The depression of
the cricothyroid membrane is identified above the
superior margin of the cricoid cartilage (fig. 4-26).
Make a small lateral incision at the base of the thyroid
cartilage to expose the cricothyroid membrane. Excise
this membrane (taking care not to go too deeply) and
insert a small-bore air line into the trachea.
4-28
Figure 4-25.—Proper insertion of suction tip.
Figure 4-26.—Anatomical structures of the neck to identify
the cricothyroid membrane.