and the back of the hands will be hard to
distinguish.
There are frequent complaints of thirst. Even the
severely wounded may complain of thirst rather
than pain.
The kidneys may shut down. Urine formation
either ceases or greatly diminishes if the systolic
blood pressure falls below 80 for long periods of
time.
The person may faint from inadequate venous
blood return to the heart. This may be the result
of a temporary gravitational pooling of the blood
associated with standing up too quickly.
HYPOVOLEMIC SHOCK
Hypovolemic shock is also known as oligemic or
hematogenic shock. The essential feature of all forms
of hypovolemic shock is loss of fluid from the
circulating blood volume, so that adequate circulation
to all parts of the body cannot be maintained.
Hemorrhagic Shock
In cases where there is internal or external
hemorrhage due to trauma (hemorrhagic shock), there
is a loss of whole blood, including red blood cells. The
diminished blood volume causes a markedly lessened
cardiac output and reduced peripheral circulation.
This results in reduction of oxygen transported to the
tissues (hypoxia); reduction of perfusion, the
circulation of blood within an organ; and reduction of
waste products transported away from the tissue cells.
Under these conditions, body cells are able to carry on
their normal functions for only a short period of time.
The body tries to restore the circulatory volume by
supplying fluid from the body tissues. The result is a
progressive fall in the hematocrit (ratio of red blood
cells to plasma) and in the red blood cell count.
Burn Shock
In burn shock, on the other hand, there is a
progressive increase in the hematocrit and red blood
cell count. This increase is due to hemoconcentration
from loss of the plasma fraction of the blood into and
through the burned area.
NEUROGENIC SHOCK
Neurogenic shock, sometimes called vasogenic
shock, results from the disruption of autonomic
nervous system control over vasoconstriction. Under
normal conditions, the autonomic nervous system
keeps the muscles of the veins and arteries partially
contracted. At the onset of most forms of shock,
further constriction is signaled. However, the vascular
muscles cannot maintain this contraction indefinitely.
A number of factors, including increased fluid loss,
central nervous system trauma, or emotional shock,
can override the autonomic nervous system control.
The veins and arteries immediately dilate, drastically
expanding the volume of the circulatory system, with a
corresponding reduction of blood pressure.
Simple fainting (syncope) is a variation of
neurogenic shock. It often is the result of a temporary
gravitational pooling of the blood as a person stands
up. As the person falls, blood again rushes to the head,
and the problem is solved. Neurogenic shock may also
be induced by fear or horror, which will override the
autonomic nervous system control.
Shell shock and bomb shock are other variations of
neurogenic shock that are important to the Hospital
Corpsman.
These are psychological adjustment
reactions to extremely stressful wartime experiences
and do not relate to the collapse of the cardiovascular
system. Symptoms range from intense fear to complete
dementia and are manifestations of a loss of nervous
control. Care is limited to emotional support of the
patient and his evacuation to the care of a psychiatrist
or psychologist.
4-23
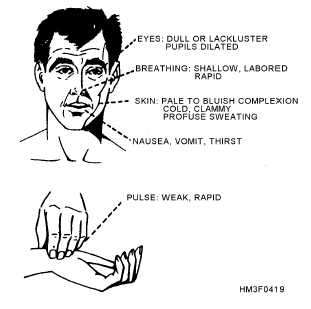
Figure 4-19.—Symptoms of shock.