12 inches (fig. 13-7). You must consider the type of injury before deciding on the position. The casualty's injuries may prevent you from using the standard position. For example, if a person with a chest wound has trouble breathing, you will raise the head slightly, and place the patient in a sitting or semi-sitting position. If a casualty is vomiting or bleeding around the mouth, place the patient on the side or back with the head turned to one side and lower the feet. If the face is flush rather than pale, or if you have any reason to suspect head injury, do not raise the feet. Instead, keep the head level with or slightly higher than the feet. If the casualty has broken bones, you must judge the best position for both the fractures and for shock. A fractured spine must be immobilized before the casualty is moved at all to avoid further injuries. A helpful mnemonic: If the face is red, raise the head; if the face is pale, raise the tail (feet).
Conserve Body Heat. - Loss of body heat can cause shock to develop or to become worse. Keep the casualty warm. Cover the patient with blankets or any dry material. Do not overheat the casualty.
Relieve Pain. - Pain is a major cause of shock. Treatment of injuries will often reduce pain. Pain may also be relieved by slightly repositioning the casualty. Under mass casualty conditions, you may have to administer morphine to certain types of casualties to relieve pain. The condition under which morphine may be administered will be discussed in the Morphine Administration section. Morphine must never be administered if there is evidence of severe or worsening shock.
Injuries to Bones, Joints, and Muscles
Injuries to bones, joints, and muscles are some of the most common situations that you will encounter. These injuries can range from the simple to the critical and life threatening. Whether the injury is mild or severe, your ability to provide quick and efficient emergency care may prevent further pain and injury.
An essential part of em emergency treatment for fractures consists of immobilizing the injured part with splints so the sharp ends of broken bones will not move around and cause further damage to nerves, blood vessels, or vital organs. Splints are also used to immobilize severely injured joints or muscles and to prevent the enlargement of extensive wounds. You must have a general understanding of the types and uses of splints.
SPLINTS. - Whether ready made or improvised, splints must fulfill certain requirements. They should be lightweight, but must be strong and fairly rigid. They should be long enough to reach the joints above and below the fracture.
Splints should be wide enough so that the bandages used to hold them in place will not pinch the injured part. Splints must be padded on the sides that touch the body; if they are not properly padded, they will not fit well and will not adequately immobilize the injured part. If you have to improvise the padding for a splint, you can use articles of clothing, bandages, cotton blankets, or any other soft material. If the casualty is wearing heavy clothes, you may be able to apply the splint on the outside, allowing the clothing to serve as part of the required padding.
To apply a splint to an injured part, fasten it in place with bandages, strips of adhesive tape, articles of clothing, or any other available material. If possible, one person should hold the splint in position while another person fastens it. Figure 13-8 shows a properly placed splint for a fractured femur.
Although splints should be applied snugly, they should never be tight enough to interfere with blood circulation. Remember to leave the fingers or toes exposed. If the tips of the fingers or toes become blue or cold, you will know that the splint or bandages are too tight. You should examine a splinted part approximately every half hour, and loosen the fastenings if the circulation appears to be impaired.
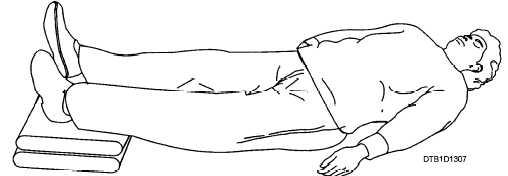
Figure 13-7. - Position of casualty for treatment of shock.
Continue Reading