consciousness as the head is lowered, which improves the blood supply to the brain. Signs and symptoms of heat exhaustion are similar to those of shock; the victim will appear ashen gray, the skin cool, moist, and clammy and the pupils may be dilated (fig. 4-75). The vital signs usually are normal; however, the victim may have a weak pulse, together with rapid and shallow breathing. Body temperature may be below normal.
Treat heat exhaustion as if the victim were in shock. Move the victim to a cool or airconditioned area. Loosen the clothing, apply cool wet cloths to the head, axilla, groin, and ankles, and fan the victim. Do not allow the victim to become chilled (if this does occur, then cover with a light blanket and move into a warmer area). If the victim is conscious, give a solution of 1 teaspoon of salt dissolved in a liter of cool water. If the victim vomits, do not give any more fluids. Transport the victim to a medical treatment facilit y as soon as possible. Intravenous fluid infusion may be necessary for effective fluid and electrolyte replacement to combat shock.
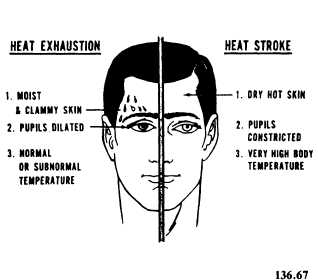
Figure 4-75 .—Heat exhaustion and heat stroke.
Heat Stroke
Sunstroke is more accurately called heat stroke since it is not necessary to be exposed to the sun for this condition to develop. It is a less common but far more serious condition than heat exhaustion, since it carries a 20 percent mortality rate. The most important feature of heat stroke is the extremely high body temperature (105°F, 41°C, or higher) accompanying it. In heat stroke the victim suffers a breakdown of the sweating mechanism and is unable to eliminate excessive body heat build up while exercising. If the body temperature rises too high, the brain, kidneys, and liver may be permanently damaged.
Sometimes the victim may have preliminary symptoms such as headache, nausea, dizziness, or weakness. Breathing will be deep and rapid at first, later shallow and almost absent. Usually the victim will be flushed, very dry, and very hot. The pupils will be constricted (pinpoint) and the pulse fast and strong (fig. 4-75). Compare these symptoms with those of heat exhaustion.
When providing first aid for heat stroke, remember that this is a true life-and-death emergency. The longer the victim remains overheated, the more likely irreversible brain damage or death will occur. First aid is designed to reduce body heat fast.
Reduce heat immediately by dousing the body with cold water or by applying wet, cold towels to the whole body. Move the victim to the coolest possible place and remove as much clothing as possible. Maintain an open airway. Place the victim on his or her back, with the head and shoulders slightly raised. If cold packs are available, place them under the arms, around the neck, at the ankles, and in the groin. Expose the victim to a fan or air conditioner, since drafts will promote cooling. Immersing the victim in a cold water bath is also very effective. If the victim is conscious, give cool water to drink. Do not give any hot drinks or stimulants. Discontinue cooling when the rectal temperature reaches 102°F; watch for recurrence of temperature rise by checking every 10 minutes. Repeat cooling if temperature reaches 103 rectally.
Get the victim to a medical facility as soon as possible. Cooling measures must be continued while the victim is being transported. Intravenous fluid infusion may be necessary for effective fluid and electrolyte replacement to combat shock.
Prevention of Heat Exposure Injuries
The prevention of heat exposure injuries is a command responsibility, but the medical department plays a role in it by educating all hands about the medical dangers, monitoring environmental health, and advising the commanding officer.
On the individual level, prevention centers on water and salt replacement. Sweat must be replaced ounce for ounce; in a hot environment, water consumption must be drastically increased. Salt should be replaced by eating well-balanced meals, three times a day, salted to taste. In the field, “C” rations contain enough salt to sustain