Local anesthesia of the maxilla will diffuse readily through the periosteum and bone to the nerves supplying the teeth, but the greater density of the cortical bone in the mandible makes diffusion more difficult. Some lower front teeth may be anesthetized by an infiltration injection, but the lower posterior teeth will generally require nerve block anesthesia. Techniques for the administration of nerve block anesthesia are described in the Cooke-Waite Manual of Local Anesthesia.
Before administering an intraoral injection, wipe the injection site free of saliva and debris. Swab the area with a Betadine sponge. Whenever possible, avoid multiple injections in the oral cavity. By carefully analyzing the location of the teeth you want to anesthetize, you will normally be able to block the area with a single injection.
Place the patient in a recumbent or supine position for the injection. Reassure the patient about the procedure to help calm him or her and to avoid syncope. Never leave a patient alone following an injection. Do not inject into an area of swelling and inflammation. When swelling or other indication of soft tissue inflammation exists, the nerve may be blocked central to the area of inflammation.
The most commonly used anesthetic for dental injections is Iidocaine (HCL) or Xylocaine® in a 2 percent aqueous solution. Xylocaine with 1:100,000 epinephrine may be used to prolong the anesthetic effect. Use a 23- to 27-gauge 1-inch nee- dle for all infiltration injections; however, a 23- to 25-gauge 1 5/8-inch needle may be required for some regional blocks.
Xylocaine is a relatively nontoxic preparation. The maximum safe dose for an adult is 300 mg. Toxic reactions may be the result of either exceeding the maximum safe dose or injecting the anesthetic intravenously faster than the body can detoxify it. Always remember to aspirate before injecting the anesthetic. A toxic reaction to Xylocaine may have a brief excitatory stage followed by depression or may simply be evidenced by respiratory and cardiac depression. Cerebral anoxia may precipitate convulsions. Most toxic reactions are mild and transitory. Place the patient in a supine position, and ensure that there is a clear airway and adequate oxygen. Support the respiratory and cardiac functions until the body can detoxify the drug, thus ending the reaction. Unless an extreme overdose has been administered, the reaction will be brief and transitory and require no medications. Other possible reactions to look for when administering intraoral injections are hematomas, blanching of the skin, temporary paralysis of facial muscles, and sometimes loss of eye control and temporary blindness. These reactions will usually disappear as the drug is detoxified by the body.
ORAL DISEASES AND INJURIES
As is true of all diseases and injuries, the symptoms discussed here refer to what the patient describes and the signs pertain to what you observe.
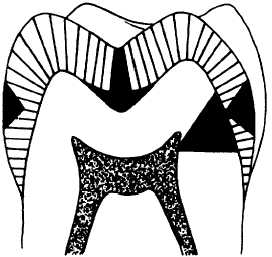
Figure 2-6.-The progress of caries: Caries in the enamel (left); caries going through the enamel and into the dentin (top); caries spreading along the dentin-enamel junction and going through the dentin to involve the pulp (right).
Dental Caries
This is the most widespread chronic disease of mankind. The most common cause of dental caries is bacterial plaque. The plaque on a tooth gives bacteria a place to breed. These bacteria release acids and other toxins that attack tooth enamel. This produces carious lesions (cavities).
Dental caries destroys tooth tissues. Caries begins in the enamel. Usually, it first appears as a chalky white spot on the enamel. It may stop there, but if it does not, it goes through the enamel and into the dentin. As the caries goes farther into the dentin, the tooth pulp may be affected. Figure 2-6 shows how caries progresses into the