5. Upon the direction of a medical officer, start an intravenous line.
REMOVING FOREIGN OBJECTS
Many wounds contain foreign objects. Wood or glass splinters, bullets, metal fragments, bits of wire, fishhooks, nails, tacks, cinders, and small particles from grinding wheels are examples of the variety of objects or materials that are sometimes found in wounds. In some cases, first aid treatment for wounds includes the removal of such objects when they are near the surface and exposed. However, first aid treatment does not include the removal of deeply embedded objects, powdered glass, or any widely scattered material of this nature. You should never attempt to remove bullets, but you should try to find out whether the bullet remains in the victim; look for both entrance and exit wounds. The general rule to remember is this: Remove foreign objects from a wound when you can do so easily and without causing further damage; but NEVER HUNT FOR OR ATTEMPT TO REMOVE DEEPLY BURIED OR WIDELY SCATTERED OBJECTS OR MATERIALS except in a definitive care environment.
The following procedure may be used to remove a small object from the skin or tissues if the object is near the surface and clearly visible:
1. Cleanse the skin around the object with soap and water and paint with any available skin antiseptic solution.
2. If necessary, pierce the skin with a sharp instrument (a needle, razor, or sharp knife that has been sterilized by passing it through a flame several times).
3. Grasping the object at the end, remove it. Tweezers, small pincers, or forceps maybe used for this purpose. (Whatever instrument you use should first be sterilized by boiling if at all possible.)
4. If the wound is superficial, apply gentle pressure to encourage bleeding.
5. Cover the wound with a dry, sterile dressing.
If the foreign object is under a fingernail or toenail, you may have to cut a V-shaped notch in the nail so that the object can be grasped by the forceps. Do not try to dig the object out from under to nail with a knife of similar instrument.
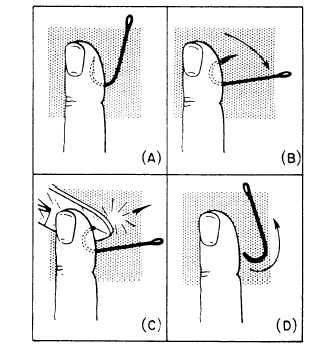
Figure 4-49.—Removing a fishhook.
A curved or barbed object such as a fishhook may present special problems. Figure 4-49 shows one method of removing a fishhook that has become embedded in the flesh. As you can see from figure 4-49A, the barb on the hook prevents its direct removal. However, if you push the hook forward through the skin, as shown in figure 4-49B, you can clip of the barb with a wire cutter or similar tool, as shown in figure 4-49C. The remainder of the fishhook can then be withdrawn in the manner indicated in figure 4-49D.
WOUND CLOSING
The care of the wound is largely controlled by the tactical situation, facilities available, and the length of time before proper medical care maybe available. Normally, the advice to the corpsman regarding suturing of wounds would be DO NOT ATTEMPT IT. However, if days are to elapse before the patient can be seen by a surgeon, the corpsman should know how to use the various suture procedures and materials and how to select the most appropriate of both.
Before discussing the methods of coaptation (bringing together), some of the contraindications to wound closing should be described:
1. If there is reddening and edema of the wound margins, infection manifested by