help lift the victim, they can accomplish the job without too much movement of the victim’s body, but a smaller number of people should NEVER attempt to lift the victim.
5. Evacuate the victim very carefully.
Fracture of the Pelvis
Fractures in the pelvic region often result from falls, heavy blows, and accidents that involve crushing. The great danger in a pelvic fracture is the organs enclosed and protected by the pelvis may be seriously damaged when the bony structure is fractured. In particular, there is danger that the bladder will be ruptured. There is also danger of severe internal bleeding; the large blood vessels in the pelvic region may be torn or cut by fragments of the broken bone.
The primary symptoms of a fractured pelvis are severe pain, shock, and loss of ability to use the lower part of the body. The victim is unable to sit or stand. If the victim is conscious, there may be a sensation of “coming apart. ” If the bladder is injured, the victim’s urine may be bloody.
Do not move the victim unless ABSOLUTELY necessary. The victim should be treated for shock and kept warm but should not be moved into the position ordinarily used for the treatment of shock.
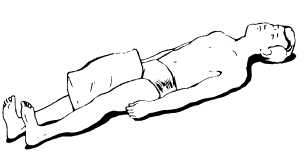
Figure 4-62.—Immobilizing a fractured pelvis.
If you must transport the victim to another place, do it with the utmost care. Use a rigid stretcher, a padded door, or a wide board. Keep the victim supine. In some cases, the victim will be more comfortable if the legs are straight while in other cases the victim will be more comfortable with the knees bent and the legs drawn up. When you have placed the victim in the most comfortable position, immobilization should be accomplished. Fractures of the hip are best treated with traction splints. Adequate immobilization can also be obtained by placing pillows or folded blankets between the legs as shown in figure 4-62 and using cravats, roller bandages, or straps to hold the legs together, or through the use of MAST garments. Fasten the victim securely to the stretcher or improvised support and evacuate very carefully.
INJURIES TO JOINTS AND MUSCLES
Injuries to joints and muscles often occur together, and sometimes it is difficult to tell whether the primary injury is to a joint or to the muscles, tendons, blood vessels, or nerves near the joint. Sometimes it is difficult to distinguish joint or muscle injuries from fractures. In case of doubt, ALWAYS treat any injury to a bone, joint, or muscle as though it were a fracture.
In general, joint and muscle injuries may be classified under four headings: (1) dislocations, (2) sprains, (3) strains, and (4) contusions (bruises).
Dislocations
When a bone is forcibly displaced from its joint, the injury is known as a DISLOCATION. In some cases, the bone slips back quickly into its normal position, but in other cases it becomes locked in the new position and remains dislocated until it is put back into place. Dislocations are usually caused by falls or blows but occasionally by violent muscular exertion. The most frequently dislocated joints are those of the shoulder, hip, fingers, and jaw.
A dislocation is likely to bruise or tear the muscles, ligaments, blood vessels, tendons, and nerves near a joint. Rapid swelling and discoloration, loss of ability to use the joint, severe pain and muscle spasms, possible numbness and loss of pulse below the joint, and shock are characteristic symptoms of dislocations. The fact that the injured part is usually stiff and immobile, with marked deformation at the joint, will help you distinguish a dislocation from a fracture. In a fracture, there is deformity BETWEEN joints rather than AT joints, and there is generally a wobbly motion of the broken bone at the point of fracture.
As a general rule, you should NOT attempt to reduce a dislocation —that is, put a dislocated bone back into place—unless you know that a medical officer cannot be reached within 8 hours. Unskilled attempts at reduction may cause great damage to nerves and blood vessels or actually