Proper placement of the anesthesia should result in a loss of sensitivity in a few minutes. This is tested by asking the patient if he or she can distinguish a sharp sensation or pain when a sharp object is gently applied to the skin.
Obtaining local anesthesia is similar except you are anesthetizing nerves immediately adjacent to where you will be working and not nerve trunks. There are two generally accepted methods of infiltrating the anesthesia. One is through the skin surrounding the margin of the wound and the other is through the wound into the surrounding tissue. In either case, sufficient quantities must be infiltrated to effect anesthesia approximately 1/2 inch around the wound, taking care not to inject into a vein or artery.
A note of caution: The maximum recommended amount of Xylocaine to be used is 50 cc for a 1 percent solution or the equivalent.
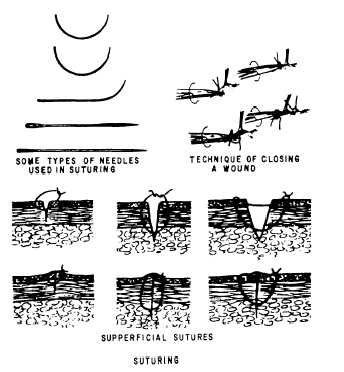
Figure 4-50.—Suturing.
General Principles of Wound Suturing
Wounds are closed either primarily or secondarily. A primary closure is within a short time of when the wound occurred; a secondary closure is a delayed closure for up to several days. In general, wounds less than 6 hours old can be closed without the danger of infection. Wounds 6 to 14 hours old may be closed if they are not grossly contaminated and are meticulously cleaned. Wounds 14 to 24 hours old should not be closed primarily. When reddening and edema of the wound margins, discharge of pus, persistent fever, or toxemia are present, do not close the wound. Do not close primarily a large, gaping, soft tissue wound. This type of wound is certain to contain large quantities of bacteria. These wounds will require warm wet dressings and irrigations, along with aseptic care for 3 to 7 days to clear up the wound. Then a delayed wound closure may be performed.
1. Debride the wound area and convert circular wounds to elliptical ones before suturing. Circular wounds cannot be closed with satisfactory cosmetic result.
2. Try to convert a jagged laceration to one with smooth edges before suturing it. Make sure that not too much skin is trimmed off that would make the wound difficult to approximate.
3. Use the correct technique for placing sutures. The needle holder is applied at approximately one quarter of the distance from the blunt end of the needle. Suturing with a curved needle is done toward the person doing the suturing. Insert the needle into the skin at a 90 degree angle and sweep it through an arclike motion, following the general arc of the needle.
4. Carefully avoid bruising the skin edges being sutured. Use Adson forceps and very lightly grasp the skin edges. It is improper to use dressing forceps while suturing. Since there are no teeth on the grasping edges of the dressing forceps, the force required to hold the skin firmly may be enough to cause necrosis.
5. Do not put sutures in too tightly. Gentle approximation of the skin is all that is necessary. Remember that postoperative edema will occur in and about the wound, making sutures tighter. See figure 4-50.
6. If there is a significant chance that the sutured wound may become infected (e.g., bites, delayed closure, grossly contaminated), place a small iodoform or rubber drain in the wound and remove it in 48 hours.
7. When suturing, the best cosmetic effect is obtained by using numerous interrupted simple sutures placed 1/8 inch apart.