system, it has the advantages of providing greater air volume (up to 4 liters per breath), and being far easier to use since both hands can be used to maintain the airway and keep the mask firmly in place (fig. 4-15).
TECHNIQUE.— Standing behind the head of the victim, open the airway by tilting the head backward. Place the mask over the victim’s face (for adults, the apex goes over the bridge of the nose; for infants, the apex fits over the chin, with the base resting on the bridge of the nose). Form an airtight seal for the mask and keep the airway open by pressing down on the mask with both thumbs while using the other fingers to lift the jaw up and back. The corpsman then ventilates into the open chimney of the mask.
Oxygen can be added by hooking the valve up to an oxygen supply. Since the oxygen flow will be diluted by the rescuer’s breath in artificial ven- tilation, the flow rate will have to be adjusted to increase oxygen concentration. At 5 liters per minute, the oxygen concentration will be approx- imately 50 percent. At 15 liters per minute, this will increase to 55 percent.
The mask has an elastic strap so it can be used on conscious self-ventilating patients to increase oxygen concentration.
Esophageal Obturator Airway (EOA)
An EOA is a semi-flexible large-bore tube ap- proximately 30 cm in length, with 19 holes in the shaft and an inflatable cuff. A soft face mask is attached to one end and the other end is closed. The airway was designed for personnel who are not authorized to place endotracheal tubes. One of the distinct advantages is that it can be inserted blindly through the mouth without having to visualize the larynx. It is also helpful in the preven- tion of gastric regurgitation. The disadvantages are that the tracheo-bronchial tree cannot be ade- quately suctioned and there is the possibility of esophageal rupture when the cuff is inflated too fully.
The following steps are to be followed when inserting the EOA:
1. Hyperventilate the patient.
2. Position the head in a neutral position or slightly flexed. DO NOT hyperextend the neck.
3. Lift the jaw as in figure 4-16A.
4. Insert the tube until the mask is flush with the face as in figure 4-16B.
5. Ventilate through the tube and auscultate both lung fields. The EOA is sometimes in- serted into the trachea; this is of little worry if recognized and corrected immediately.
6. Inflate the cuff (about 35cc of air). Overinflation can possibly rupture the esophagus or may compress the trachea causing an obstruction.
7. Ventilate and auscultate again to ensure proper placement.
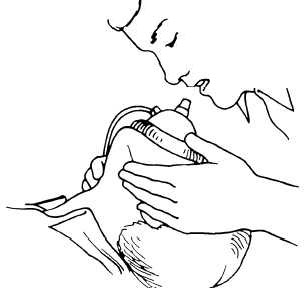
Figure 4-15.—Mouth-to-mask breathing.
Cricothyroidotomy
A cricothyroidotomy, often known as an emergency tracheotomy, consists of incising the cricothyroid membrane, which lies just beneath the skin between the thyroid cartilage and the cricoid cartilage. The cricothyroid membrane can be located easily in most cases. Hyperextend the neck so that the thyroid notch (Adam’s apple) becomes prominent anteriorly. Identify the posi- tion of the thyroid notch with the index finger. This finger descends in the midline to the promi- nence of the cricoid cartilage. The depression of the cricothyroid membrane is identified above the superior margin of the cricoid cartilage (fig. 4-17). A small lateral incision is made at the base of the thyroid cartilage to expose the cricothyroid mem- brane. This membrane is then excised, taking