amount of time elapsed, and the constitution of the casualty, you may have to reassign priorities. What appears to be a minor wound on initial evaluation may develop into a profound shock, or a casualty that requires immediate treatment may be stabilized and down-graded to a delayed status.
SORTING FOR EVACUATION
During the Vietnam war, the techniques of helicopter medical evacuation (MEDEVAC) were so improved that most casualties could be evacuated to a major medical facility within minutes of their injury. This considerably lightened the load of the hospital corpsman in the field, since provision for long-term care before the evacuation was not normally required. However, rapid aeromedical response did not relieve the corpsman of the responsibility for giving the best emergency care within the field limitations in order to stabilize the victim before the helicopter arrived. Triage was seldom a problem since most of the injured could be evacuated quickly.
New developments in warfare, along with changes in the probable theaters of deployment, indicate that the helicopter evacuation system may no longer be viable in a front-line environment. If this becomes the case, longer ground chains of evacuation to the BAS or division clearing station may be required. This will increase the need for the life stabilizing activities before each step in the chain and in transit. Evacuation triage will normally be for personnel in the Class II and Class III treatment categories, based on the tactical situation and the nature of the injuries. Class IV casualties may have to receive their treatment at the BAS level and Class I personnel would be treated on the line.
Remember, triage is based on the concept of saving the maximum number of personnel possible. In some cases, a casualty has the potential to survive, but the treatment necessary requires a great deal of time and supplies. As difficult as it may be, you may have to forsake this patient in order to save others that have a greater potential for survival.
BASIC LIFE SUPPORT
Basic life support is the emergency techniques for recognizing and treating failures of the respiratory system and heart function. The primary emphasis is placed on maintaining an open AIRWAY to counter upper airway obstruction; restoring BREATHING to counter respiratory arrest; and restoring CIRCULATION to counter cardiac arrest. These are the ABC’s of basic life support.
UPPER AIRWAY OBSTRUCTION
The assurance of breathing takes precedence over all other emergency care measures. The reason for this is simple: If a person cannot breathe, he or she cannot survive.
Many factors can cause the patient’s airway to become fully or partially obstructed. In the adult, a very common cause of obstruction is improperly chewed food that becomes lodged in the airway; the so-called “cafe coronary.” Children have a disturbing tendency to swallow foreign objects during play. Another cause occurs during unconsciousness, when the tongue may fall back and block the pharynx (fig. 4-1). Normally, the heart will continue to beat until oxygen deficiency becomes acute. Periodic checks of the carotid artery must be made to ensure that circulation is being maintained.
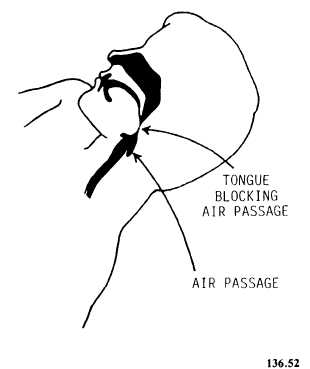
Figure 4-1.—Blocked airway.