finger. Take a deep breath and seat your lips around the
patient’s mouth (creating an airtight seal), and give two
slow ventilations (1 ½ to 2 seconds per breath). See
figure 4-11. Allow enough time for the lungs to deflate
between ventilations. If the patient still does not
respond, continue mouth-to-mouth ventilations at the
rate of 10 to 12 ventilations per minute or one breath
every 5 seconds. Periodically, check the pupils for
reaction to light; constriction is a sign of adequate
oxygenation.
NOTE: When performing artificial ventilation
and the lungs cannot be inflated adequately,
repeat head tilt-chin lift or jaw-thrust
maneuver, and again attempt ventilation. If the
lungs still do not inflate adequately, assume the
airway is obstructed by a foreign object.
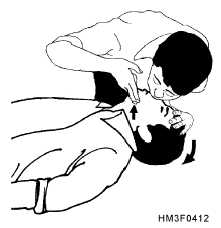
M O U T H - T O - N O S E . — M o u t h - t o - n o s e
ventilation is effective when the patient’s mouth
cannot be opened (lockjaw), extensive facial or dental
injuries occur, or an airtight seal of the mouth cannot be
achieved. Figure 4-12 shows an example of this
procedure.
To administer this technique, tilt the head back
with one hand on the patient’s forehead and use the
other hand to lift the jaw (as in the head tilt-chin lift
maneuver). Close the victim’s mouth. Take a deep
breath, seal your lips around the patient’s nose, and
give two ventilations. Allow the victim’s lungs to
deflate passively after each ventilation. If the victim
does not respond, then you must fully inflate the lungs
at the rate of 10 to 12 ventilations per minute or one
breath every 5 seconds until the victim can breathe
spontaneously.
MOUTH-TO-STOMA.—A casualty who has
had surgery to remove part of the windpipe will breathe
through an opening in the front of the neck called a
stoma. Cover the casualty's mouth with your hand,
take a deep breath, and seal your mouth over the stoma.
B r e a t h e s l o w l y, u s i n g t h e p r o c e d u r e s f o r
mouth-to-mouth breathing. Do not tilt the head back.
(In some situations, a person may breathe through the
stoma as well as his nose and mouth. If the casualty’s
chest does not rise, cover his mouth and nose, and
continue breathing through the stoma.)
MOUTH-TO-MASK.—The mouth-to-mask
breathing device includes a transparent mask with a
one-way valve mouth piece.
The one-way valve
directs the rescuer’s breath into the patient’s airway
while diverting the patients’s exhaled air away from
the rescuer. Some devices have an oxygen adaptor that
permits the administration of supplemental oxygen.
4-17
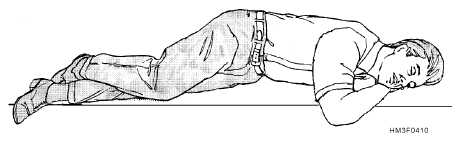
Figure 4-10.—A patient in the recovery position.
Figure 4-11.—Mouth-to-mouth ventilation.
Figure 4-12.—Mouth-to-nose ventilation.